Rochelobe
-
Posts
221 -
Joined
-
Last visited
Content Type
Profiles
Forums
Events
Articles
Media Demo
Everything posted by Rochelobe
-
So despite evidence that cloth masks offer reductions around 40 to 50% in transmission (vs N95s which are more like 90% reduction), you say they do nothing at all. Despite evidence, in the research paper I quoted that shows that they DO reduce the transmission. 40% reduction is worthless? Well, in that case, why does any citizen ever need a weapon. I can be fully armed walking down the street and someone can pop up from a rooftop with a rifle and shoot me without my ever seeing them. Or a plane could drop a bomb on me. Thus, my weapons are worthless right? There is no point in a "worthless" self defense tool that doesn't stop all possible situations, right? Again - masks were used in Europe to reduce the spread (even cloth masks) and they have managed to restart sports, and in the case of Australia, they have even started allowing attendance. This does not define a path to success for you? Do you only want normal situations with 90,000 fans crammed into Memorial Stadium? After all, since N95 masks are not even 100%, they are useless as well since some people are going to catch the disease. Very few preventative medical procedures promise 100% safety or perfection, so I guess they should all be ceased. I can brush my teeth every day and still get cavities, so what's the point. Clearly the toothbrush/tooth paste do no good at all. All I want (in the context of this thread) is for people to wear masks to help reduce the spread, improve the ability to identify and isolate positive cases, and allow us to have some college football. Why does the solution have to work 100% in order to be implemented? Very few things work 100% of the time.
-
I agree that masks do not stop the spread. That is not the purpose. Slowing the spread != Stopping the spread. I guess what I don't understand is the massive resistance as if somehow masks make all live unlivable. As far as 1918 - approximately ~675K Americans died during that pandemic, out of a population of ~106M. Since we are at around 3 times that number of Americans today, following the same approaches used during the 1918 pandemic would result in a around ~2M American deaths due to coronavirus, assuming the death rate is the same. Estimates I've seen for the Spanish flu mortality rate have been as high as 2.5%. At this time we have a mortality rate of 6% for coronavirus worldwide. I realize we may be missing a bunch of asymptomatic cases, meaning coronavirus isn't that deadly, but, since we only have the current data, we don't yet have any "strong science" to support a lower death rate, so I guess we have to go with what the current numbers are for a mortality rate based upon current deaths and positive cases. A lower number is only inferred, correct? Also in 1918 vs 2020 is that schools had nothing remotely close to the liability attached to them in 1918 if athletes got sick/died as we would have in 2020. Lawyers have fundamentally changed how institutions will have to deal with this, even outside of the medical information. There can be positive and negative benefits due to this increased scrutiny, but in this case it probably leads to an increasing chance of the season being cancelled. I doubt the same types of legal protections were in place for players in 1918. For good or for bad that is probably the dominant reason the season will be cancelled. The virus could be raging, but if there was any way the schools knew they would be legally protected, I think we'd be having a very different discussion - more about how teams would cope with missing players, but the expectation would be the season would proceed.
-
I was using cloth masks in mid-April. I started using crude folded bandannas cut from a T-shirt around 1 Apr, ~2 weeks after my state issued their stay-at-home order. Some kind of covering was required if you wished to enter grocery stores at that time. By ~13 Apr I was able to find and start using cloth masks with ear holders. "Strong science" Are you are saying there is no published research on the use of cloth masks? http://files.fast.ai/papers/masks_lit_review.pdf From the abstract of the same paper: This paper was published in April 2020. At that time a mask recommendation was considered scientifically valid. https://www.ucsf.edu/news/2020/06/417906/still-confused-about-masks-heres-science-behind-how-face-masks-prevent https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-mask/art-20485449 I doubt the Mayo Clinic is going to recommend cloth masks without having seen some metrics that support their use in reducing spread of the virus. https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover-guidance.html https://www.kpax.com/news/how-cloth-face-mask-reduce-covid-spread Yeah, there is no scientific evidence at all. Are cloth masks in and of themselves a complete solution? NO Is anyone saying they are a complete solution? NO Who is (generally) saying that they should not be used? (In my opinion) Those using political, rather than medical agendas as their driving point. Once again - the idea is to slow the spread as much as possible in order to buy time for proactive quarantining rather than bulk quarantining of everyone. Europe has used cloth masks in conjunction with social distancing and heavy testing as they have decreased their rate of active positive cases. They still have hot spots flaring up, so we must continue to work for a vaccine. Masks are meant to help us buy time. Most of the rest of the world resumed sports sooner than the US, and has been able to start allowing attendance at some of those sporting events (AFL). The US may try that in September with college football, but, based upon current infection rates, it will probably hasten the shutdown of the season unless things seriously improve, such as an order of magnitude or more reduction in daily positives. Bottom Line: In my opinion, the United States missed the opportunity to sufficiently contain the initial wave of the virus during the months of April/May/June, which would have lowered the daily new positive rate low enough that a feasible college football season could have occurred in the Sep-Dec time frame. At this point, evidence would indicate that we will not sufficiently lower counts anytime in the near future, unless we become more diligent about mask use. So, if a season does occur under the current situation it will probably be greatly disrupted by outbreaks, with many teams playing (at most) 3 or 4 games this fall.
-
I doubt Fauci feels it is an end all strategy either. Now that we have several months of data, there is evidence that wearing a mask lowers the chance of transmission. I think the thrust is as follows: 1. Wear masks: Wearing masks lowers the transmission rate, slowing the spread of the virus (but not stopping it all by itself). 2. Increase testing: Increased testing should provide a more complete snapshot of how widespread the infection is, particularly the asymptomatic cases that apparently can spread the virus without ever being aware they have the virus. 3. Expanded testing processing: Expanded processing lowers the amount of time people wait to get results after they are tested. Advantages of using all three in combination: a. Slowing transmission rate allows for hospitals to "space out" the number of COVID patients they have at any given time, thus allowing them to provide better treatment, resulting in a (hopefully) lower rate of death. b. Slowing transmission rate with increased testing/expanded processing allows for a chance to get ahead to better identify potential hotspots prior to being fully realized. Thus, to me the logical steps at that time would be to use the combination of the three methods to more quickly identify those with the virus earlier in the process - and find the asymptomatic cases and quarantine them - instead of having to quarantine everyone. However, those out and about in society should still use masks to slow the rate, so that the spread can be limited until we can turn around, say 30% or more tests per day in a given community (with much quicker turnaround times, hopefully only a day or so). I think by doing that we would be able to slowly stamp it down (probably not out), and at least buy time for a vaccine. At the same time, it allows for more opening of a communities businesses as the positive rate drops, and those that are positive are more quickly identified and quarantined. Had we started implementing this in mid-April, we would most likely have a semi-normal college football season this fall - maybe with 20-40% attendance. I just watched an Australian Rules Football match Saturday night (our time) that had fans in the stands. Probably 15% attendance. I believe Australia implemented procedures similar to the ones I listed above.
-
I know they are not a football league, but yet another conference dropping all non-conference games: https://omaha.com/sports/college/creighton/big-east-goes-conference-only-for-fall-sports-no-decision-on-basketball-yet/article_a02eed44-18e3-5d6d-9445-79f53621d65c.html This entire exercise (going conference only, minor conferences canceling fall sports), feels like slow motion dominoes that will eventually knock over fall P5 football.
-
That information does seem hard to find. Of course, with HIPAA, the players would have to consent to releasing that they tested positive. My guess (pure speculation) is not many, possibly none of them showed symptoms. If a huge cluster of players were showing symptoms I think it would have been much bigger news.
-
Yes, and they seem to be having success. However, they have already had two teams withdraw (FC Dallas and Nashville SC) - Dallas had 11 players test positive and Nashville had 9. A few other games have been postponed due to positive cases. And this is for players in an isolation bubble. Unless they are just going to lock down all the college football players for the entire fall, I think we will see many more teams have to withdraw or postponement/cancellation of games. Not impossible to work through, but we could see a lot of teams with 4 game seasons spread out over 3 months, or similar types of chaos.
-
On the Beach?
-
"Will there be a 2021 football season?"
-
Yes, I think there is evidence that the risk is lower in lower population density areas. That is probably not a surprising result. However, what does seem to be indicated, no matter where we are is that large numbers of people, gathered in close proximity, seems to greatly increase the spread. This is the situation in bars. There have been several cases of bars/restaurants being responsible for hot spots. At this time there doesn't seem to be a large indication that the protests have been as bad - even though those are also high density events. To me the main difference is (1) the majority of protestors are wearing masks while those in bars/restaurants are not and (2) the protests are outside while the documented bar/restaurant hot spots have taken place indoors. So which matters more? Probably being indoors with non-filtered recirculated air. But, I'm not sure we can completely discount the impact masks have had on reducing spread during the protests. It could be simply that the outdoor environment with UV+wind disperses things better, but it might also be the combination of masks reducing the amount of aerosols. So where would football be in this scenario? I could see arguing both ways - football is close proximity thus dangerous or football is (primarily) outdoors and thus lower risk. I've seen the face shield plans and I'm not sure how effective those would be vs masks at reducing aerosol propagation during an athletic event. I think we end up with no football primarily because we won't have enough evidence in a month or so to show that risk is much lower than indoor dining. I hope I am wrong and we can have football this fall, I'm just not very optimistic.
-
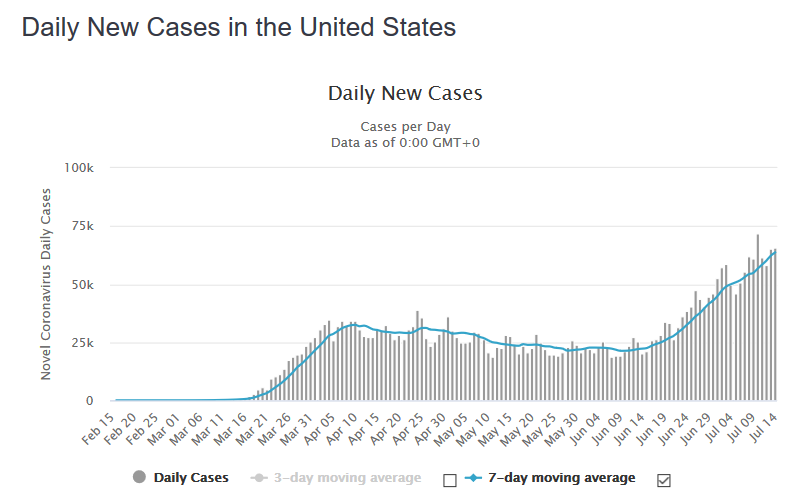
Looking at the worldometer site for daily new cases supports your point - the uptick in positive cases dates from early/mid June, right around 4 weeks ago. Some of the people that have died have died quickly - I've read a few stories where someone started feeling bad and within a few days they were gone. However, I've seen more stories of people that had a slow decline that pushed them to the hospital, then spent weeks on a ventilator before dying - which is more aligned with the 4 weeks from exposure to death scenario. As far as the sudden declines go, it could be they were exposed and pre-symptomatic/mild for 2 weeks or more prior to their quick decline. The next 3 weeks could be really bad (as in peak in New York/Italy bad). Some things that might mitigate that - (1) average age of those hospitalized is going down, and maybe younger people that get really sick will have a high probability of recovering (2) as the pandemic has progressed there are signs that doctors are finding ways to mitigate the effects of the virus in some patients, improving their chance for recovery. (3) the virus may have mutated into a less lethal form (even as it seems it may have mutated into a more communicable form) I don't think we have enough evidence to be definitive on any of these possibilities, so I think it is reasonable to say we are still in a very high risk environment, until we see if any of the things listed above are actually happening. The timeline for determining any of these factors does not match up well with the planned start of the football season.
-
Because, apparently its just like WWII, I guess. https://www.usatoday.com/story/sports/ncaaf/2020/07/10/lou-holtz-fox-news-normandy-college-football-season/5414975002/ I understand what he means about risk, but its always a lot easier to say that when the speaker doesn't have to take the risk. Later, regarding the Big Ten's move to conference only for this season: Skip Holtz coaches at La Tech, so I guess that is why he picked them. I just thought it was funny that he picked a team that has its non conference P5 matchups against two conferences (Big XII, SEC) that haven't yet moved to conference only schedules.
-
I think this is a key point. Most Athletic Departments at large universities deal with serious coin, involving hundreds of employees, players, and support personnel. By going conference only, it provides control over scheduling the games which is crucial to maximize flexibility for TV broadcasts. In a scenario with empty (or very low allowed attendance) stadiums, the TV money will be even more critical this season than in a normal season.
-
-
Since Notre Dame has the agreement with the ACC for ~5 games a year, I saw a couple of stories speculating that they may just end up playing all ACC teams this year - since ACC may want to not abandon their agreement with Notre Dame this year in hopes of keeping it going forward when things return to "normal". I think it would be good to bring in Notre Dame for a year, but would they also want one more team to keep it at an even number of teams so they don't have to have mandatory idle weeks? Of course that's the same issue the ACC faces if they bring in Notre Dame for the year.
-
Did you mean respond with text? Ok, square peg in a round hole to your plan. Or you are attempting to put a conventional wisdom idea into a totally different view. You are using typical hope and potential delusion into a totally different problem with too many different variables. Is this satisfactory? I did not ask the question "Thoughts?" I assume you understand that word was in my post because I was quoting another poster. Or, were you just trying to troll me but cut all of my response?
-
Your trolling might be more effective if you actually responded to the person that asked the question.
-
I think these (particularly 3 and 4) seem like a good compromise if we have good progress on lowering the number of positive cases by mid Oct. 3 and 4 also have the advantage of probably not really affecting the fall 2021 season, if things have started getting back to pre-COVID days.
-
Until it is definitive on what, if any season happens for this fall, I would doubt we hear much. Once we see what kind of season there will be I would assume a few possibilities: 1) No season - eligibility extended, similar to how NCAA handled spring sports 2) ~10 game seasons (conference only) - most likely business as usual as far as eligibility 3) Truncated season (schedule is interrupted, most teams only play 2 or 3 games) - Who knows? One solution for possibility 3 would be to treat it similar to the redshirt rule and say no one had the opportunity to play enough games, so eligibility is extended. Or they could treat it like the way basketball was treated - you got your season, so no eligibility extension. Of course there is a difference in this scenario vs basketball, where the regular season was completed, just not the post season. Possibility 2 is more similar to how the 2019-2020 Basketball season was handled. Maybe if the season is truncated they try to come back in the spring to finish or play a few games. Spring practice with actual games on the weekends, or something like that.
-
Men's Hoops non-conference schedule released
Rochelobe replied to knapplc's topic in Husker Basketball
In light of the Big Ten making all fall sports conference only, what impact does this have on the non-conference basketball schedule? Is basketball considered a winter sport without any changes (at this time) even though these games would still be played when it is technically fall? -
Sorry everybody for again taking the thread off topic. I'll stop posting on this issue in this thread, since it doesn't seem to be making any impact anyway.
-
Yes, Doctors have learned about this virus in the past few months. All I have been saying is that by extending the timeline, they have the opportunity to develop treatments which can result in a net drop in loss of life. To me this is important if we don't have a vaccine for a few years. At this time, there is still not definitive evidence that herd immunity is going to be meaningful for this particular virus. https://www.ibtimes.com/coronavirus-treatment-drug-banned-sports-found-effective-fighting-covid-19-3006779 https://www.theatlantic.com/ideas/archive/2020/07/why-covid-death-rate-down/613945/ Also, the herd immunity approach doesn't mean the economy just keeps chugging along: https://theweek.com/speedreads/924238/sweden-literally-gained-nothing-from-staying-open-during-covid19-including-no-economic-gains https://www.marketwatch.com/story/sweden-didnt-impose-a-lockdown-its-economy-is-just-as-bad-as-its-neighbors-who-did-2020-06-25 I agree - it sucks what has happened to the economy. A lot of people are going to be evicted over the next month or so, simply because their job evaporated due to the lockdown. Small businesses will be lost. College towns are going to have severe impacts this fall due to the lack of home football games. However, there is a compromise between complete lockdown and completely being opened. Its called masks and social distancing. Does it solely resolve the problem? No. But it is an important contributing factor to allow us to work through two competing interests. 1) Keep economy chugging along 2) Protect citizens Using masks and social distancing buys time for doctors to find a way to at least improve survival rates of those hospitalized - which evidence indicates they are having measurable success at. At the same time, masks and social distancing, while still being an imposition, are certainly less impactful on the economy than a complete shutdown. Why do you feel the only solution is absolutely no restrictions? At this point, herd immunity has not shown much promise. https://www.bloomberg.com/news/articles/2020-06-17/sweden-proves-surprisingly-slow-in-achieving-herd-immunity Granted we are still learning about immunity to this new disease, but at this point the evidence is indicative of no herd immunity until the vaccine is available. This is possibly due to the fact that this is a new virus, and our body doesn't know what to do with the antibodies. Even worse, natural antibodies may actually worsen the impact: https://www.newsweek.com/coronavirus-antibodies-body-brain-damage-1516828 Granted, many of these studies are in the early stages. The point is doctors need time to figure this out. Stretching things via masks/social distancing is about the only method we have that still allows us to keep an operational economy.
-
This guy seems a bit miffed at the Big Ten's decision: https://www.usatoday.com/story/sports/college/2020/07/09/big-10-football-cancels-nonconference-games-2020-ramifications-coronavirus/5410182002/ I guess this columnist feels it is the responsibility of the large schools to make sure the small schools' athletic programs are funded. That would be true, to an extent if the NCAA was like the NFL, NBA, MLB, etc. If universities were "franchises" within the NCAA Football League. But the organization is only an association. The closest thing to a league concept are conferences. At the end, the point is probably moot for this year, since the chance the whole season just gets canceled is probably increasing each day. There is validity to the fact that the P5 does push the rest of the teams around. I wonder what % of athletic money is generated by the P5 schools vs the other ~200 non-P5 Division 1 schools across all sports.
-
I agree. Sweden went for the herd immunity approach. The results: 7359 cases/million, 545 deaths/million For comparison, the US is currently at 9723 cases/million, 410 deaths/million Other Scandinavian countries (which followed more formal lockdowns/masking/social distancing): Denmark: 2230 cases/million, 105 deaths/million Finland: 1313 cases/million, 59 deaths/million Norway: 1653 cases/million, 46 deaths/million Since May 31: Norway is averaging <10 new positive cases/day, Finland is averaging ~40 new positive cases/day (down to <10 since mid June) Denmark is averaging ~35 new positive cases/day Sweden is averaging ~1000 new positive cases/day Sweden actually had a surge in June, and just in the last week or two they've finally started to drop. Provided doctors can develop treatments, wide open herd immunity would kill a lot more people than masking/social distancing: (1) too many sick at once - hospitals can't do proper treatment (2) not enough time to develop mitigating treatments However, if your goal is to maximize the number of victims, herd immunity is a great solution
-
Seriously!?!?!!? Improving treatments which improve survival means no additional lives saved? So no medicine anywhere that ever saves anyone from dying is actually worth it, since the patient will eventually die anyway (from old age if nothing else) So, I have a situation where I know 10000 people will get the virus. Scenario 1: I do nothing to stop the spread and all 10000 get it in the first month, with a death rate of 5%, meaning 500 people die. Of course your fanciful herd immunity thing is in effect. Scenario 2: I enforce wearing masks, doing social distancing, etc and instead of all 10000 getting it the first month, we spread it out over 10 months, with 1000 per month getting it. During that time, doctors learn about various techniques/medicines that are able to mitigate many of the bad effects of the virus. So as each month goes by, there is a slight decrease in the death rate, say from 5% the first month down to 1% by the 10th month. So lets assume the average is 3% over the 10 months. In that situation only 300 people die. There is evidence that doctors are learning about treatments that can lower the death rate. While not proven yet, it could really help with lowering the overall number of deaths, at the cost of making the period of masking/social distancing go on for longer. I guess the people that are saved in scenario 2 are not important to you. When the hospitals overflow in scenario 1, who gets to decided who lives and who dies (who gets treatment and who doesn't)?